COPD Evaluations
"The dilemma in the Canadian health-care system is that we can't admit them [chronic obstructive pulmonary disorder patients] all. We don't have enough beds."
"We [his research team] were trying to come up with a risk score to predict who was at risk of doing poorly so we could be more accurate in identifying those who needed [hospital] admission."
"That's sort of a trade-off [increased hospital admissions] we'll have to deal with if we want the best outcomes for our patients."
"You have to put it together [social factors], discuss it with the patient and family, and make a recommendation as to whether or not to go home. It's a tool that makes our care safer for people."
"An emergency department is a crazy place to work [within]. You have huge numbers of people coming in the door 24/7, and they all have different problems. But some of these problems we see time after time after time, and it's now possible to systematize and standardize assessments in a way that wasn't done before."
Dr. Ian Stiell, Emergency Room physician, senior scientist, The Ottawa Hospital
 COPD, an umbrella term for a number of diseases including chronic
bronchitis and emphysema, is a chronic disease caused largely by smoking
and characterized by shortness of breath, cough and sputum production.
It progresses slowly over many years. As it advances, shortness of
breath limits the activity levels of individuals and reduces their
quality of life. It can also lead to premature death. Council of Academic Hospitals of Ontario
COPD, an umbrella term for a number of diseases including chronic
bronchitis and emphysema, is a chronic disease caused largely by smoking
and characterized by shortness of breath, cough and sputum production.
It progresses slowly over many years. As it advances, shortness of
breath limits the activity levels of individuals and reduces their
quality of life. It can also lead to premature death. Council of Academic Hospitals of OntarioDr. Stiell is recognized across the global medical community for his work in producing data to drive rule-making within hospital settings. Guidelines to assist emergencv room doctors have been developed by him, so ER physicians are enabled logically to determine when medical tests should be prescribed for knee injuries, concussions and spinal injuries, as well as a risk scale for heart failure. More recently he has been instrumental in producing a new study to demonstrate how an assessment tool can be of immeasurable help to emergency-room doctors required to make critical decisions about how to respond to patients with breathing difficulties.
Patients experiencing difficulties breathing as a result of chronic obstructive pulmonary disorder (COPD) are frequent visitors to hospital emergency rooms, presenting doctors with a dilemma. COPD is a serious disease of the lungs that is often attributed to smoking. The condition can be severely aggravated with the onset of a simple cold or flu, leaving COPD patients struggling for air with their compromised lungs. Faced with such patients, doctors on duty must arrive at a decision whether to admit patients to hospital or to send them back home after treatment, based on their assessment.
Dr. Stiell, with his immense experience as a seasoned ER physician emphasizes the importance for patients and hospitals that the correct COPD patients -- those most likely to develop dangerous complications -- be admitted. Emergency doctors have relied on their experience and clinical judgment in the past, along with consultations on occasion, when they reach their informed determinations. But that decision-making can be fraught with the potential for deleterious results arising on occasion.
About 38 percent of COPD patients in Canada were admitted to hospital after arrival at an emergency department with shortness of breath, according to earlier research published by Dr. Stiell. Many of those presenting with such symptoms have been sent home following their assessment and treatment, and among them some patients suffered seriously compromising events, the result of which was that some of these patients died. This is an obviously critical issue requiring a solution.
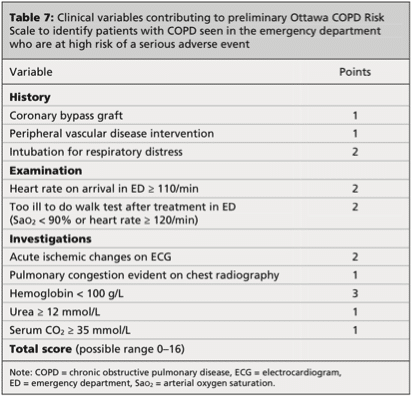
So together with his research team Dr. Stiell examined medical data arising out of 945 COPD cases to identify the common characteristics of high-risk patients which they then used to develop a ten-point "risk scale" to be used by ER doctors to more accurately identify those patients who are most likely to develop dangerous complications. The study tested the validity of the risk scale based on the experience of ER doctors from six Canadian hospitals, and it was published in the Canadian Medical Association Journal.
The finding was that through employment of the features identified in the scale, emergency-room physicians were enabled to improve their predictions significantly to identify which patients were likely to suffer dangerous complications in the short term. A total of 1,415 COPD patient records were studied. Of that number, 135 had suffered serious setbacks in the month following their visit to an emergency room. Using conventional assessment methodology 52 percent of cases were correctly predicted for serious complications. With the use of the risk scale that number jumped to 79.3 percent correct predictions.
What resulted from that increased accuracy, predictably, was a modest hospital admission increase. Dr. Stiell is satisfied that the COPD scale presents doctors with an objective measure of the risk faced by patients with COPD, a score that is not considered in isolation of social factors, as, for example, whether the patient has access to a caregiver and family doctor.

Labels: Best Practice, Chronic Obstructive Pulmonary Disorder, COPD, Emergency Room Physicians, Hospitals, Research
posted by Pieface @ 6:29 PM
![]()
![]()

0 Comments:
Post a Comment
<< Home